Procedure
Following patient preparation (as for spinal), ‘loss of resistance' technique is used to locate the epidural space. A midline lumbar epidural is shown below: for non-midline and non-lumbar approaches, see the reference text Wildsmith, Armitage and McClure (2002).
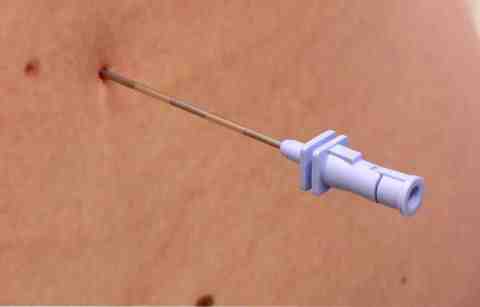
Stage 1
The epidural needle is inserted into the skin in the midline, at the midpoint of the chosen interspace, and its obturator removed. In this case, the operator has removed the detachable wings. There is no consensus on the best way to hold needle and syringe. Considerable variation in technique exists.
Following patient preparation (as for spinal), ‘loss of resistance' technique is used to locate the epidural space. A midline lumbar epidural is shown below: for non-midline and non-lumbar approaches, see the reference text Wildsmith, Armitage and McClure (2002).
Stage 2
A syringe is attached to the needle. Using a syringe of saline is most common, although some prefer to use air. (See Tab ‘Saline or air?’). When the needle tip is in the ligamentum flavum, the syringe plunger is rigid - total resistance is felt. Advancing a fraction further, sudden loss of resistance is felt, signalling the needle tip's entry into the epidural space. Advancement stops and the needle depth is noted, denoting the skin to space distance.

Following patient preparation (as for spinal), ‘loss of resistance' technique is used to locate the epidural space. A midline lumbar epidural is shown below: for non-midline and non-lumbar approaches, see the reference text Wildsmith, Armitage and McClure (2002).
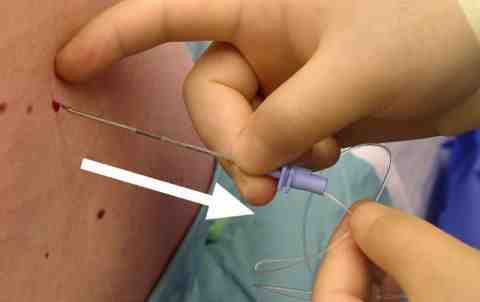
Stage 3
The catheter is then threaded through the needle until an appropriate length is in the space (5 cm is an appropriate length to leave). There should be no severe or persistent pain, although transient pain in root distribution can sometimes occur.
Following patient preparation (as for spinal), ‘loss of resistance' technique is used to locate the epidural space. A midline lumbar epidural is shown below: for non-midline and non-lumbar approaches, see the reference text Wildsmith, Armitage and McClure (2002).
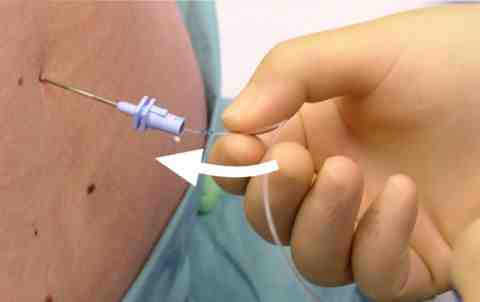
Stage 4
The needle is withdrawn carefully whilst the catheter is held firmly in place to prevent its withdrawal. If necessary the catheter can then be further withdrawn.