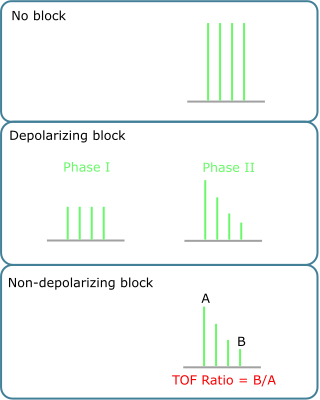
The depth of neuromuscular blockade can be assessed using the TOF (Fig 1). The number of muscle twitches corresponds approximately with the receptor occupancy. The majority of operations require no more than 90% receptor occupancy by a neuromuscular blocking agent. However, the diaphragm is relatively resistant to neuromuscular blockade, so that a TOF count of one may well be present with diaphragmatic movement which may interfere with gastric surgery.
If reversal of neuromuscular blockade is attempted prematurely then the degree of muscle power regained may not be adequate.
Reversal should be complete prior to the patient regaining consciousness. If the patient is able to lift their head for five seconds, they are demonstrating a sustained tetany, suggesting complete reversal. Any degree of fade indicates incomplete reversal. Breathing does not indicate adequate reversal.
Visual assessment of muscle twitches to a PNS is subjective and often unreliable. Three actions help to reduce residual neuromuscular blockade during recovery (Fig 2).